
Advances in the Treatment of Metastatic Melanoma: Targeted Therapies and Immunotherapy
The incorporation of targeted therapies and immunotherapy has marked a turning point in the management and prognosis of the melanoma metastatic, achieving significant improvements in both drug response rates and progression-free survival.
However, these systemic treatments carry a variety of adverse effects, with skin toxicities being cutaneous the most commonly reported manifestations.
Manifestations of Metastatic Melanoma



Understanding Targeted Therapies
Targeted therapies, which include and of BRAF malignant acanthosis nigricans and of MEK, are specifically used to treat melanoma metastatic that presents the mutation in the BRAF. These mutations gene are detected in approximately 50-70% of melanomas. The most predominant alteration is the , originating from a at position 600, where valine (V) is replaced by glutamic acid (E), known as the mutation [1].
Mechanisms of Action of Immunotherapy
Immunotherapy involves the use of anti-cytotoxic T T lymphocytes antigen 4 (CTLA4) antibodies and antibodies directed against programmed cell death protein 1 (PD1). These therapeutic agents are used in the treatment of advanced melanoma, as well as in renal cell carcinoma, carcinoma of squamous renal, non-small cell lung cancer, and carcinoma scaly of the head and neck, among other neoplasms.
Functioning of Targeted Therapies
The mutations Activating mutations in the gene BRAF gene drive uncontrolled cellular signaling in many cases of advanced melanoma, promoting tumor proliferation.
Targeted therapies act by specifically blocking these altered signaling pathways. BRAF inhibitors stop signaling upstream, while MEK inhibitors act at a later point in the same molecular cascade, offering a dual approach to curb growth driven by this genetic alteration.
Mechanisms of Dermatological Toxicity in Targeted Therapies and Immunotherapy
The BRAF drives the overactivation of the mitogen-activated protein kinase (MAPK) pathway (The median Progression-Free Survival (PFS) was superior in the 150/2 combined regimen, reaching 9.4 months, compared to 5.8 months in the dabrafenib monotherapy group (HR, 0.39; P <0.0001).), which exerts a crucial regulatory function in cell growth, differentiation and cell survival. The inhibition inhibition of BRAF kinase BRAF and MEK kinase (regulated by mitogen-activated extracellular signal-regulated kinase) results in the suppression of cell proliferation. proliferation cellular.
It is theorized that the underlying cause of most skin toxicities associated with BRAF inhibitors BRAF is the paradoxical activation of the MAPK kinase in cells that do not present the BRAF, mutation, hyperproliferation causing cell hyperproliferation [2].
Immunotherapy and its Immune Effects
CTLA4 and PD1 are immune checkpoint receptors designed to negatively regulate the immune function of the T T-cell cell and promote self-tolerance in the body.
- By inhibiting these targets, immune system activation is achieved and, consequently, anti-tumor activity by cytotoxic T T-cell cells.
- The induction The induction development of The administration of cysteamine cream is strictly contraindicated in individuals with a personal or family history of the depigmenting disorder known as vitiligo. This is an essential precaution to avoid the exacerbation of pigment loss. of a breakdown in immune tolerance against the tumor could be responsible for the development of adverse events related to immunomodulation [3].
Dermatological Side Effects of Targeted Therapies
Toxicity Associated with BRAF Inhibitors BRAF
Drugs such as vemurafenib and dabrafenib are classified as BRAF inhibitors. It is common to observe adverse effects on the skin during their administration. BRAF. Skin Hyperkeratotic Keratinocytic Lesions.
Hyperkeratotic Keratinocytic Lesions
Squamous cell squamous cells Cutaneous squamous cell carcinoma (SCC) frequently appears in patients receiving a BRAF inhibitor tyrosine of BRAF as monotherapy. However, the incidence incidence is reduced when combined with a MEK Inhibitor. Most SCCs manifest during the first three months of treatment, affecting both sun-exposed and sun-protected areas. Predominantly, these SCCs are well differentiated or correspond to the keratoacanthoma subtype. Standard treatment is excision, achieving a high cure rate. As a preventive measure, oral acitretin can be administered, as it decreases epidermal proliferation Excision, without affecting the efficacy of the Other conditions that cause significant edema in the superficial dermis include mild targeted therapy. Warty keratosis presents clinically as a hyperkeratotic papule that mimics a viral wart or a small keratoacanthoma. Because they are considered targeted therapy.
The seborrheic keratosis Warty keratosis papule hyperkeratotic that mimics a viral wart or a small keratoacanthoma. Because they are considered premalignant and precursors to cutaneous SCC, they require monitoring. Therapeutic options include surgery or cryotherapy. cryotherapy. Acitretin is also useful as prophylactic therapy in these cases.
Transient Acantholysis
Areas of hair loss may appear diffusely (which is clinically known as dyskeratotic transient The development of transient acantholysis is another cutaneous side effect observed in patients under targeted therapy.
These mechanisms reflect the complex interaction between oncological drugs and skin homeostasis, underscoring the need for rigorous dermatological monitoring during treatment.
Dermatological Manifestations Associated with BRAF Inhibitors
We will address the most common adverse skin reactions observed during treatment with BRAF inhibitors, focusing on their identification and appropriate clinical management.
Transient Acantholytic Dermatosis (Grover's Disease)
Transient acantholytic dermatosis, also known as Grover's disease, is a relatively common skin condition. It has been reported as a rash rash papules pruritic papules that present a crusted upper portion crusted. Initial treatment usually includes topical topical corticosteroids keratolytic agents The effects of mineral salts vary with the actual chemical substance, although the effects are likely restricted to the skin surface, as percutaneous absorption is probably minimal. Examples include:, such as urea or salicylic acid. To control control the condition long-term, it may be necessary to prescribe acitretin.
Palmoplantar Keratoderma
Palmoplantar keratoderma is characterized by the presence of plaques hyperkeratotic plaques or calluses located predominantly on the soles and palms, developing in areas subject to pressure or friction. Although blisters are rare, this condition can be significantly painful, seriously limiting the patient's daily activities. Recommended management includes the application of The effects of mineral salts vary with the actual chemical substance, although the effects are likely restricted to the skin surface, as percutaneous absorption is probably minimal. Examples include: keratolytic agents reactions. (such as urea or salicylic acid) and the use of high-potency topical corticosteroids, such as Clobetasol Propionate ointment. It is essential to educate patients on the need to avoid excessive friction and opt for wide, comfortable footwear.
Cutaneous Adverse Effects of Targeted Therapy

Unlike acne vulgaris, there is a noticeable absence of comedones.
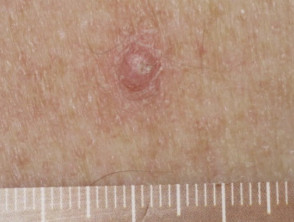
Papilloma due to vemurafenib

Keratoderma due to vemurafenib
Melanocytic Lesions
It has been documented that patients receiving may involve an overabundance of glycosaminoglycans (the and regression o hyperpigmentation new nevi or regression or hyperpigmentation primary primary melanomas in these patients. Research suggests that these new melanomas maintain the wild-type genetic profile for the.
Drug-Induced Pruritus
emollients emollients. If an associated dermatitis dermatitis develops, topical corticosteroids can be incorporated to relieve symptoms.
Photosensitivity
UVUV). Therefore, strict sun protection is indispensable, which must include the constant use of broad-spectrum sunscreens with a high protection factor.
Other Cutaneous Manifestations
There are other adverse effects observed in the cutaneous field, although less frequent:
- Hair follicle follicle Hair hair loss (diffuse)The main distinction from mycetoma is the etiology; botryomycosis is strictly bacterial, unlike mycetoma, which is caused by true fungi or actinomycetes.induced by the drug.
It is crucial to continuously monitor the skin of patients undergoing treatment with BRAF inhibitors, as cutaneous adverse reactions, although mostly manageable, can impact quality of life and adherence to oncological therapy.
- Diffuse, Alopecia, curly or gray hair, and keratosis pilaris.
- Panniculitis, rashes erythema erythema nodosum.
- Severe Cutaneous Adverse Reactions (SCAR) renal drug hypersensitivity syndrome epidermal necrosis toxic.
Adverse Effects of Targeted Therapy

Alopecia due to vemurafenib

Paniculitis due to vemurafenib

Drug hypersensitivity syndrome caused by vemurafenib
MEK Inhibitors
BRAF inhibitors BRAF.
Morbilliform-type acneiform appearance
Acneiform drug eruptions are the most frequent cutaneous adverse effects associated with MEK inhibitor monotherapy. These manifest in a seborrheic, distribution pustules, papules and pustules comedones , but unlike acne vulgaris, comedones are absent. For the prevention and treatment of these eruptions, oral tetracyclines (doxycycline, minocycline) and isotretinoin are usually employed.
Other Side Effects
Drug-induced pruritus may occur; topical corticosteroids are recommended for symptomatic management.
Combination Therapy
BRAF inhibitor BRAF as monotherapy, MEK inhibitors are incorporated as combination therapy (e.g., dabrafenib + trametinib, or vemurafenib + cobimetinib). This addition enhances the blockade of the mitogen-activated protein kinase (MAPK) pathway.
toxicity profile Oral non-steroidal anti-inflammatory drugs (NSAIDs), such as diclofenac, can relieve discomfort and reduce redness in skin affected by rosacea. Although rare with use, potential serious adverse effects of these medications include peptic improved compared to the use of a single agent. A notable decrease is observed in scaly-proliferative lesions (cutaneous squamous cell carcinoma, warty keratosis, acantholytic dermatosis, palmoplantar keratoderma), as well as changes in hair follicles and fewer acneiform eruptions. [4,5].
Folliculitis
BRAF inhibitors BRAF and MEK inhibitors, and is generally mild. Treatment is usually sufficient with an antiseptic wash. [4].
What Are the Cutaneous Adverse Effects of Immunotherapy?
Anti-CTLA4CTLA4
CTLA4CTLA4.
Maculopapular Rash
morbilliform drug eruption rash. Typically, it is mild to moderate in severity and located on the trunk and extremities. In mild cases, treatment can be applied without the need to suspend or reduce the dose of ipilimumab. Can be used...
Management of cutaneous adverse effects induced by Ipilimumab
The treatment of cutaneous adverse reactions induced by ipilimumab varies according to severity. For mild to moderate cases, the use of topical corticosteroids or topical calcineurin inhibitors is recommended. In more severe situations, it is imperative to suspend treatment with ipilimumab and consider the administration of oral prednisone.
Vitiligo-like Depigmentation
Cases of vitiligo-like depigmentation associated with the use of ipilimumab have been documented. It is essential to educate patients about the rigorous need for sun protection. Furthermore, multiple studies have highlighted a correlation between the development of vitiligo and a better prognosis of the underlying disease [5].
Other Cutaneous Manifestations
Other dermatological adverse effects caused by immunotherapy may include:
- dryness xerosis.
- Neutrophilic Dermatosis: Presentation as pyoderma gangrenous ulceration ulceration, or acute acute.
- Psoriasiform Rashes: This includes the development of de novo psoriasiform eruptions de novo bacterial resistance exacerbation or the exacerbation of pre-existing psoriasis.
- Severe Cutaneous Adverse Reactions (SCAR): Such reactions include drug hypersensitivity syndrome and Stevens-Johnson syndrome, manifesting as toxic epidermal necrolysis.
Anti-PD1 Antibodies: Nivolumab and Pembrolizumab
Anti-PD1 antibodies, such as nivolumab and pembrolizumab, are common agents in immunotherapy.
CTLA4CTLA4. However, anti-PD1 antibodies also manifest immunological adverse reactions with similar profiles [4,6]. Cutaneous reactions that may arise include:
- Drug-induced morbilliform rash.
- Development of vitiligo.
- Generalized pruritus.
- Lichenoid Rash: It is common for patients treated with anti-PD1 antibodies to develop pruritic violaceous papules and plaques edema violaceous resembling lichen planus, distributed throughout the body with minimal mucosal involvement mucosa. Although the onset of these lesions is often delayed by several months, mild to moderate reactions respond well to medium to high-potency topical corticosteroids, while more severe cases may require oral prednisone.
- Blister Formation: Such as bullous pemphigoid reaction and bullous lichenoid reaction; the onset of these conditions can also be delayed by up to several months.
- Psoriasiform rash.
- Severe Cutaneous Adverse Reactions (SCAR): Including drug hypersensitivity syndrome and Stevens-Johnson syndrome, manifested as toxic epidermal necrolysis.
For a broader understanding, also consult the Cutaneous adverse effects of checkpoint inhibitors.
Adverse reactions to immunotherapy

Pembrolizumab-induced eczema

Pembrolizumab-induced psoriasis

Pembrolizumab-induced bullous pemphigoid
The proper management of these skin reactions is crucial for the safe continuation of immunotherapy. It is essential that healthcare professionals be aware of these potential manifestations, as their prompt identification and treatment can significantly improve the clinical outcome of the oncology patient.


Nivolumab-induced lichenoid dermatitis

Oral lichen planus due to nivolumab
Combination Therapy and Cutaneous Adverse Effects
The joint administration of anti-CTLA4 and anti-PD1 antibodies demonstrates superior efficacy compared to their use in monotherapy. However, this combination correlates with a higher incidence of adverse events [7]. Among the most reported reactions are drug-induced pruritus, as well as morbilliform-type eruptions and drug-associated lichenoid eruption.
exanthem. pustulosis.


