Understanding McCune-Albright Syndrome: Cause, Clinical Presentation, and Genetics
McCune-Albright Syndrome (MAS), initially described in 1937 and sometimes referred to as Albright Syndrome, is a rare genetic condition. It is characterized by the clinical presence of a classic triad of distinctive manifestations.
This diagnostic triad includes:
- Pigmentation skin pigmentation
- Abnormalities significant bone
- Endocrine effects, especially the premature development of puberty.
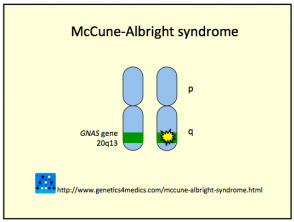
To confirm the diagnosis of MAS, it is essential that at least two of these three criteria are present. The underlying cause is a , originating from a spontaneous (randomly acquired) mutation in the gene GNAS1 gene. This genetic alteration results in an protein abnormal protein that interferes with the regulation of cell proliferation, survival, and migration. The mutation occurs in early stages of embryonic development development, affecting only a fraction of the cells (a phenomenon known as mosaicism), and most importantly, it is not heritable to the offspring of the affected patient.
Detailed Clinical Manifestations of McCune-Albright Syndrome
The clinical characteristics of McCune-Albright Syndrome are grouped based on the three primary systems affected, as summarized in the following detailed table:
| Clinical Component | Description and Specific Characteristics |
|---|---|
| 1. Irregular Skin Pigmentation |
|
| 2. Bone Abnormalities |
|
| 3. Endocrine Abnormalities |
|
| 4. Other Associated Problems |
MAS has been correlated with various additional clinical complications, including:
|
Genetic Considerations for McCune-Albright Syndrome
Understanding the genetic basis, centered on the somatic mutation of the GNAS1 gene, is crucial for the pathophysiological understanding of McCune-Albright Syndrome and the non-heritable nature of this condition.
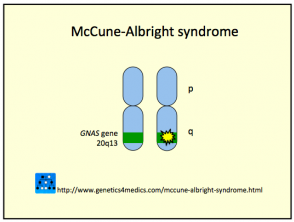
* Image courtesy of Genetics 4 Medics
Diagnosis Process for McCune-Albright Syndrome
The identification of McCune-Albright Syndrome (MAS) is based on a combination of clinical findings and specific imaging studies. Accurate diagnosis is crucial for initiating appropriate management.
- X-rays of the affected bone areas reveal distinctive features, including a central pattern cataloged as "ground glass," lytic lesions (loss of normal bone), cystic appearance, and evidence of recent or healed fractures.
- Advanced studies such as computed tomography (CT scan), magnetic resonance imaging (MRIMRI RNA) and bone scans (nuclear medicine bone scan) can be very useful supportive tools.
- Once skeletal abnormality is confirmed, it is essential to perform additional investigations to rule out endocrine abnormalities that may be present subclinically (hidden).
- Although it is feasible to perform genetic testing are being investigated. to identify the mutation, they are currently not part of the routine diagnostic protocol.
Treatment Options for McCune-Albright Syndrome
The therapeutic approach for MAS shows variable results, focusing on managing symptoms and associated complications.
- Hormonal treatment to control precocious puberty has shown uneven efficacy using various hormonal agents.
- Recently, the incorporation of bisphosphonate drugs has been tested with the goal of mitigating the frequency of fractures and relieving pain associated with bone lesions in patients with MAS; however, the results obtained so far have been inconsistent.
- Other specific endocrine dysfunctions require the implementation of individualized pharmacological treatments or surgical procedures.
Potential Complications of McCune-Albright Syndrome
The progression of bone alterations in MAS can trigger serious complications affecting various body systems.
- Bone changes affecting the skull can exert pressure on the nerves cranial nerves, possibly leading to loss of visual and/or auditory capacity.
- When bone changes are located in the rib cage, there is a risk of experiencing respiratory difficulties.
- There is a low risk, up to 2%, of developing a type of bone malignancy called osteosarcoma. This tumormalignancy tends to be more prevalent in patients who have previously received radiation therapy directed at the affected bone lesions.
- Although two long-term follow-up studies did not find a significant increase in the rate of premature mortality, several clinical reports have documented cases of sudden unexplained death in individuals with particularly severe forms of the disease.


