
Understanding Cysts: Definitions, Types, and Dermatological Causes
What Exactly Is a Cyst?
A cyst is defined as an encapsulated, round, dome-shaped lesion that is typically benign. This structure contains material that may be fluid or semi-fluid. Clinically, a cyst may feel firm or fluctuant and often causes a visible distension in the overlying skin. There are various classifications of cysts, and below we will describe the most prevalent forms.
Difference Between a Cyst and a Pseudocyst
Those cystic formations that lack a complete fibrous capsule are more accurately termed pseudocysts. These structures are common, especially in the context of acne.
Who Develops Skin Cysts?
Cysts are extremely common, affecting a minimum of 20% of the adult population. While some may be present from birth, most appear throughout life. They affect people of all ethnicities. It is important to note that for most cyst types, incidence is higher in men than in women.
Etiological Causes of Different Cyst Types
The underlying etiology of many cysts remains unknown. However, for other dermatological variants, specific origins have been identified:
- Epidermoid cysts result from the proliferation of squamous epidermal cells dermis. dermis. proliferation of epidermal cells within the dermis. Their point of origin is located in the follicular infundibulum. infiltrate, thickening at the level of the infundibulum. The presence of multiple epidermoid cysts may indicate Gardner syndrome. It is crucial to mention that the popular term "sebaceous cyst" sebaceous" is considered an inappropriate name for this condition.
- An epidermal inclusion inclusion cyst is a tissue reaction following a traumatic injury. The skin folds creating a sac that becomes lined by healthy epidermal cells that continue their cycle of multiplication, maturation, and formation of a nail edge.
- The origin of the trichilemmal cyst is established in the hair root sheath. hair. Its transmission can be autosomal dominant (due to an affected gene gene located on the short arm of chromosome chromosome 3) or present sporadically.
- In the case of the steatocystoma, its origin lies in the sebaceous duct associated with the pilosebaceous follicle duct. Multiple steatocystoma, occasionally, is a dominant hereditary disorder secondary to mutations diseases mutations located in the keratin 17 (K17) gene, which may link it to pachyonychia congenita. Most steatocysts are sporadic and do not present these mutations.
- The eruption of vellus hair vellus hair cysts autosomal dominant has its origin in the follicular infundibulum. It can be inherited as an autosomal dominant disorder due to alterations in the keratin gene.
- A dermoid cyst is classified as a hamartoma, A dermoid cyst is classified as a hamartoma development , which is essentially a developmental error.
- The origin of the ganglion cyst diseases tissue of a nearby joint.
- The obstruction The occlusion pilosebaceous units of the pilosebaceous units (the hair follicle and its associated gland) can be a cause of the formation of various cystic lesions.
Understanding the specific etiology significantly aids in differential diagnosis and in choosing the most appropriate dermatological treatment for each cyst type. cyst.
- The occlusion of the follicles follicles ducts eccrine (sweat glands) causes the accumulation of secretions, which can manifest as milia. Appearance of.
- The blockage of the opening of a mucous gland can generate a mucocele, an accumulation of fluid in a membrane pemphigoid mucous membrane, Vulva, or vagina).
- The lip, vulva, vagina). Milia , invasive extension into the deep is a pseudocyst resulting from the inability of the cutaneous appendages to release keratin. Primary primary milia sebaceous gland, is the inability of the cutaneous appendages to release keratin. Primary milia originates in the infundibulum of the vellus hair follicle, at the level of the sebaceous gland, being a reduced version of an epidermoid cyst. Secondary milia proceeds from a retention cyst within a vellus hair follicle, sebaceous duct, sweat duct, or the epidermis.
- epidermis. sebum.
Clinical Features of Dermatological Cysts
Epidermoid Cyst
- Epidermoid cysts frequently appear on the face, neck, trunk, or any area with sparse hair.
- Most of these cysts develop during adult life.
- They are more than twice as common in men as in women.
- They manifest as one or more nodules firm, round, adherent nodules, flesh-colored to yellowish, and of variable size.
- The presence of a central pore or central punctum.
- punctum is common. The keratinous content is soft, cheese-like, and has an unpleasant or foul-smelling odor. that produce a foul.
- Scrotal and labial cysts are often multiple and can occasionally calcify.
The epidermoid cyst receives other names such as follicular infundibular cyst, epidermal cyst, or keratin cyst. infundibular follicular.
Epidermoid Cyst



Gardner Syndrome
Explore additional images of epidermoid cysts to expand your knowledge.
Trichilemmal Cyst
- Trichilemmal cysts are predominantly located (90% of cases) on the scalp; although they can also appear on the face, neck, trunk, and extremities.
- The onset of most of these cysts occurs in middle age.
- In 70% of cases, trichilemmal cysts are multiple.
- They present as firm, round or oval, adherent nodules to the underlying structure.
- They lack a visible central punctum Herpetiform ulcers: They are characterized by being numerous tiny vesicles that cluster together, generally healing in approximately one month. Their most frequent location is on the surface of the tongue.
- punctum. The keratinous content is distinguished by being firm, white, and can be enucleated (extracted) easily.
The trichilemmal cyst is also known as a pilar cyst.
Trichilemmal Cyst

Pilar Cyst
Recognizing the clinical differences between the various types of cysts is fundamental for accurate diagnosis and treatment in dermatology.


Explore more images related to epidermoid cysts for better visual understanding.
Steatocystoma
- A steatocystoma that presents in isolation is called steatocystoma simplex.
- simplex. Frequently, multiple lesions lesions, armpits, (multiple steatocystoma) are observed located on the chest, arms, armpits.
- , neck, and the scrotal or vulvar region. These cysts tend to manifest at the end of adolescence and during the 20s, influenced by androgens androgens, and tend to persist persist for life.
- Clinically they are mobile, soft to pasty consistency, and yellowish, presenting as papules papules with a diameter ranging between 3 and 30 mm.
- A distinctive feature is the absence of a central point (punctum).
- The main content of the cyst is predominantly composed of sebum.
Evaluation of Multiple Steatocystoma



Eruptive Vellus Hair Cysts
- Eruptive vellus hair cysts manifest during childhood if there is a family history fever, or they present later in sporadic cases.
- They are often observed in conjunction with multiple steatocystoma.
- They are characterized by the development of multiple small papules, 2 to 3 mm, located mainly over the sternum.
- The characteristic content of these cysts includes vellus hairs.
Dermoid Cyst
- A cutaneous dermoid cutaneous cyst can contain structures derived from the skin and cutaneous appendages, and even, on occasion, include tissue such as teeth, cartilage, or bone.
- Most dermoid cysts are located on the face, neck, and scalp, frequently around the eyelid region, forehead, and glabella.
- It is a tumor thin-walled tumor with a consistency that can vary between soft and firm to the touch.
- Although the cyst originates from birth, it is not uncommon for the patient not to seek medical attention until adulthood.
Anatomy and Manifestation of Dermoid Cysts


Analyzing these various presentations of cutaneous cysts helps establish accurate differential diagnoses. The correct identification of each lesion type is fundamental, from common pilar cysts to the more complex dermoid cysts, to determine the most appropriate dermatological treatment.


Ganglion Cyst: Characteristics and Appearance
- The ganglion cyst frequently affects the scapholunate joint of the back dorsum of the wrist.
- It tends to manifest in young or middle-aged adults.
- It is significantly more prevalent in women, who present it three times more than men.
- Clinically, it appears as a firm swelling, which can be unilocular or multilocular, measuring between 2 and 4 cm in diameter, and which exhibits transillumination.
- Its main content is hyaluronic acid, a characteristically golden, viscous substance.
Visualization of the Ganglion Cyst



Digital Mucoid Pseudocyst: Clinical Manifestations
- These mucous or myxoid pseudocysts generally appear in older people, located on the distal phalanx..
- They originate from the distal interphalangeal joint associated with osteoarthritis.
- osteoarthritis. It is common for them to manifest as a longitudinal depression band over the nail, over the nail, resulting from the compression exerted on the proximal in Sneddon syndrome, affecting the trunk and back; the extremities are rarely involved..
matrix.



Images of the Myxoid Pseudocyst.
To deepen your knowledge, you can consult more images and details about these formations in our related content.Digital Mucous Cysts to Lip and Eyelid Lesions
Concluding the description of cystic lesions, we now analyze digital myxoid pseudocysts, followed by common conditions in the lips and including hidrocystomas and milia affecting the eyelid area.
Mucous or Myxoid Lip Cyst
- A cyst located on the lip generally originates from the obstruction of the salivary duct. salivary.
- This lesion is also commonly known as a mucocele.
- It typically presents as a soft to firm nodule, with a diameter ranging between 5 and 15 mm, and has a translucent.
appearance.

Lip Mucocele


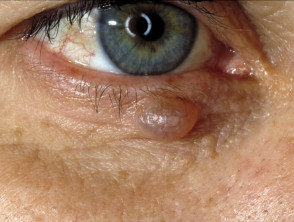
Hidrocystoma
- Mucocele of the Lip.
- Hidrocystoma.
- Hidrocystoma is defined as a translucent, gelatinous cyst that forms specifically on the eyelid. It receives other names such as cystadenoma, Moll's gland cyst, and sweat cyst. apocrine.
- The most frequent type of translucent, solitary eyelid cyst is the apocrine hidrocystoma. When multiple cysts are observed on the lower eyelid, they are classified as eccrine hidrocystomas.
- For a deeper understanding of its structure, consult the pathology pathology.
of the apocrine hidrocystoma.


Hidrocystoma of the Eyelid.
Below are additional images illustrating eyelid hidrocystomas.
- Milium / Milia.
- Milia are superficial, 1 to 2 mm, dome-shaped papules, composed of retained keratin. Primary milia are common in neonates neonates (present in 50% of cases), adolescents, and adults; they are occasionally hereditary or can present eruptively.
- In babies, primary milia affects the eyelids, cheeks, nose, the mucosa mucosa.
- (known as Epstein Pearls) and the palate (Bohn's nodules). In older children and adults, they are located on the eyelids, cheeks, and nose. Occasionally, primary milia can be observed transversely in the nasal groove or surrounding the areola.
- areola. When milia appears in a plaque, plaque lesions... , multiple lesions emerge over an.
- erythematous area impetigo, is suspected. located on the face, chin, or ears. Secondary milia appear after epidermal repair following injuries or blisters, associated with conditions such as bullous epidermolysis, bullous pemphigoid, porphyria cutanea tarda, thermal burns, and after procedures such as dermabrasion.
- The appearance of secondary milia has been documented as an adverse effect associated with the current use topical of steroids and 5-fluorouracil.
- lotion, cream, vemurafenib, and dovitinib.
Milia


Milia

Eyelid milia.
Explore image gallery of Milia.
- Vulvar Mucous Cyst.
- A vulvar mucous cyst originates from the obstruction of the Bartholin's or Skene's duct. It manifests as a soft swelling in the vaginal Presence of painless white striae arranged in a reticular pattern similar to lace or a fern. introitus. If the swelling is posterior, it is a Bartholin's cyst; if it is periurethral, it corresponds to a Skene's cyst.
Comedone and Acne Pseudocyst
- toxicity comedones Comedones.
- are considered pseudocysts created by the obstruction of the hair follicle with keratin and sebum. Open comedones (blackheads) and closed comedones (whiteheads) are superficial papules characteristic of acne vulgaris.
- Solar comedones appear on photoaged skin and are frequently related to smoking.
- In cases of nodulocystic acne and hidradenitis suppurativa, comedones are accompanied by large non-inflammatory nodular and inflammatory pseudocysts.
Images of Comedones

Open Comedones

Closed Comedones
Auricular Pseudocyst The pseudocyst of the
- auricle auricle (external ear) usually develops after localized trauma. trauma abscess.
Image of Auricular Pseudocyst
![Understanding Cysts: Definitions, Types, and Dermatological Causes What Exactly Is a Cyst? A cyst is defined as an encapsulated, round, dome-shaped lesion that is typically benign. This structure contains material that may be fluid or semi-fluid. Clinically, a cyst may feel firm or fluctuating and often causes a visible distension [...]](https://dermatly.com/wp-content/uploads/2020/11/auricular-pseudocyst__ProtectWyJQcm90ZWN0Il0_FocusFillWzI5NCwyMjIsInkiLDg1XQ.jpg)
Auricular pseudocyst
Potential Complications Associated with Cysts
Rupture of a Cyst
- The internal content of the cyst can leak through the capsular wall, causing significant irritation to the surrounding skin.
- A palpable, firm, and tender area of inflammation inflammation develops that extends beyond the original boundaries of the encapsulated cyst.
- Discharge of sterile tissue or pus.
Secondary Infection
- may occur.
Secondary Infection
- In rare cases, a cyst that has ruptured can develop a secondary infection, frequently caused by _Staphylococcus aureus_, resulting in the formation of a furuncle (a boil).
- Effects of Pressure and Compression optic.
- A dermoid cyst can exert pressure on the underlying bone, causing potential bone tissue damage. Ganglion cysts can induce joint instability, weakness, restriction of range of motion, and even compress a malformation of the nail.
nerve. A digital mucous cyst can press on the proximal nail matrix, resulting in a
- nail malformation. proliferative.
- Risk of Malignancy cancer Skin cysts and pseudocysts are intrinsically benign and non-proliferative lesions. Nodulocystic basal cell carcinoma is a common type of skin cancer that manifests as a rounded nodule. It may initially resemble a cyst, but it is distinguished by constant growth, destruction of the epidermis, and eventual ulceration and bleeding.
- ulceration and bleeding. The term "malignant proliferative trichilemmal cyst" is incorrect, as it represents an extremely rare tumor where the term does not accurately apply.
Clinical and Pathological Diagnosis of Cysts
Cysts usually present with distinctive clinical features. When a cyst is surgically removed, it is essential to subject it to histological examination. Accurate identification of the type of lining of the cystic wall and the nature of its content are crucial for the histological. pathologist pathologist to classify it correctly.
- The epidermoid cyst is lined by stratified squamous epithelium that includes a granular layer. epithelium The internal content is characterized by laminated keratin. Cysts that have ruptured may show an evident inflammatory response. granulomatous. The trichilemmal cysts lack a granular layer and present a palisaded outer layer. The content consists of eosinophilic hair keratin.
- Older cysts may show signs of calcification. The proliferating variant eosinophilic. is considered a tumor entity. calcificación. calcification. proliferate The steatocystoma is identified by a folded cystic wall with prominent lobes of associated sebaceous glands.
- A dermoid cyst encapsulates completely mature skin elements, including fat, hair, sebaceous glands, eccrine glands, and, in approximately 20% of cases, apocrine glands.
- The lining of the wall of a ganglion cyst or a digital mucous cyst is composed of collagen, nodes and fibrocytes, containing hyaline material., eccrine glands The hidrocystoma is characterized by a thin lining wall composed of bilaminar eosinophilic cells., apocrine glands.
- Treatment Options for Cysts collagen An asymptomatic epidermoid cyst hyaline.
- generally does not warrant any active treatment. It should be noted that attempting to remove only the content of a cyst, in most scenarios, leads to its.
recurrence. If the patient requires it, total excision of the cyst is the definitive option. However, recurrence is not an infrequent event, and the
excision asymptomatic may present notable surgical challenges. It is essential to remember that HNC exhibits a considerable rate of. For cysts that already present inflammation, common treatments may include: excision Incision.
Intralesional injections with triamcinolone.
- Incision Administration of oral antibiotics, if infection is suspected.
- Consider a biopsy.
- with late excision for study.
- Consider a skin biopsy Prevention of Cyst Formation.
Currently, no specific methods are known to prevent the appearance of cysts.
Long-Term Outlook for Cysts.
Cysts tend to be persistent lesions that will generally continue to exist unless complete surgical removal is opted for. Surgical excision is key to permanently resolving the condition.
cyst4__protectwyjqcm90zwn0il0_focusfillwzi5ncwymjisingildfd-9867856-1106790-jpg-3349545.


